大規模唾液調査でどうだ!
GW最後の更新はさらっと
さて、もうGWも終わりで明日からは新たな社会情勢になりそうな感じですが、なってみないとどうなりそうなのかは分かりませんよね。まあ粛々と業務をこなしていくしかないのですが、4月の収入もがた落ちで5月もなかなか厳しい状況なのはもう仕方が無いのかなと思っています。
さて、唾液中のSARS-CoV2の論文は一杯あるんですが、今日はさらっと短いやつを1本読みました。
オーストラリアの被験者数が多い論文
Saliva as a non-invasive specimen for detection of SARS-CoV-2
J Clin Microbiol. 2020 Apr 21. pii: JCM.00776-20. doi: 10.1128/JCM.00776-20.
PMID: 32317257
オーストラリアからの論文で4/21にアクセプトされています。
We further investigated the feasibility and utility of saliva collection from ambulatory patients presenting to a dedicated COVID-19 screening clinic at the Royal Melbourne Hospital (RMH), Melbourne, Australia. Between 25th March and 1st April 2020, 622 patients were tested for COVID-19 through the screening clinic. All patients had NPS, and 522/622 (83.9%) patients also provided saliva. Patients were asked to pool saliva in their mouth for 1-2 minutes prior to collection, and gently spit 1-2 mL of saliva into a 25mL collection pot. Neat saliva specimens were transported to the
27 laboratory where an approximate 1:1 ratio of liquid Amies media was immediately added. We specifically chose to use liquid Amies media in order to: (i) evaluate the use of an alternative transport media in the face of global shortages of viral transport medium (VTM), and (ii) to preserve VTM in our own laboratory. The median time from sample collection to addition of media was 180 minutes (range 55 – 537 minutes). NPS and saliva specimens underwent nucleic acid extraction on the Qiagen EZ1 platform (QIAGEN, Hilden, Germany). An extraction volume of 200uL of the sample was used, with RNA eluted in 60uL. Reverse-transcriptase PCR (RT-PCR) testing was performed using a multiplex RT-PCR test for SARS-CoV-2 and other seasonal coronaviruses (Coronavirus Typing (8-well) assay, AusDiagnostics, Mascot, Australia). All positive NPS samples for SARS-CoV-2 underwent confirmatory testing at a local reference laboratory (the Victorian Infectious Diseases Reference Laboratory) using previously published primers (3).
3月25日から4月1日までの間にCOVID-19のスクリーニングクリニックにて検査を行った622名が対象です。全ての患者には鼻咽腔綿棒による試料採取が行われています。唾液を採取したのは522名で全体の83.9%となっています。
唾液の採取方法は、採取前に1、2分程唾液を溜めておくように支持をします。その後、1~2mlの唾液を吐かせて採取します。吐唾法に近いのではないでしょうか。摂取量はあまり多くは無いですが、1,2分で2mlって結構頑張らないと出てこない気もします。(口腔外科の先生から安静時唾液の正常値は15分で1.5mlだからそんな簡単に出ないと指摘あり)その後は鼻咽腔も唾液も同じ用にRT-PCRにかけられています。
結果
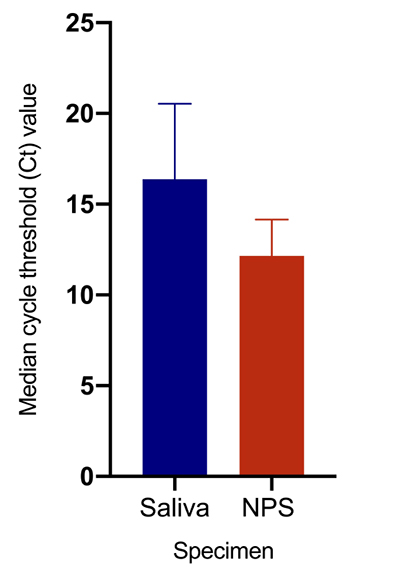
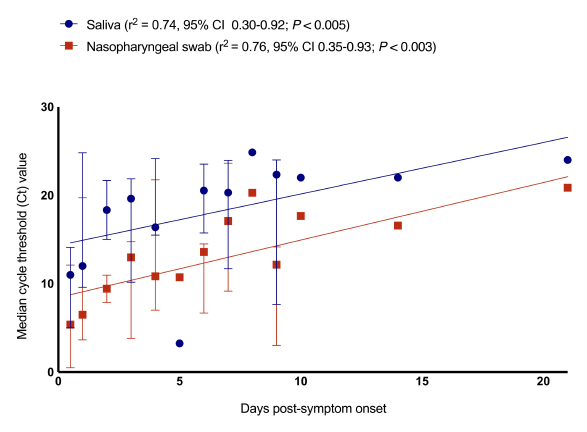
Overall, 39/622 (6.3%; 95% confidence interval [CI] 4.6%-8.5%) patients had PCR-positive NPS, and 33/39 patients (84.6%; 95% CI 70.0%-93.1%) had SARS-CoV-2 detected in saliva. The median cycle threshold (Ct) value was significantly lower in NPS than saliva (Figure 1A), suggestive of higher viral loads in NPS, and in both samples, there was a correlation between Ct value and days from symptom onset (Figure 1B). To assess specificity, a subset of saliva specimens from 50 patients with PCR negative swabs was also tested. Of note, SARS-CoV-2 was detected in 1/50 (2%; 95% CI 0.1%-11.5%) of these saliva samples, which may reflect differing quality of NPS collection.
622名中39名が鼻咽腔での検査で陽性と判定されました。その39名中33名(84.6%)に関して唾液中の検査でSARS-CoV-2が検出されました。Ct値の中央値は鼻咽腔検査の方が唾液よりも有意に低い結果を示しました。これは鼻咽腔の方がウイルス量が多いことを示唆してます。どちらの検体も症状が発現してからの日数とCt値は相関関係を示しました。鼻咽腔検査で陰性だった50人の唾液を解析したところ1例が陽性でした。これは鼻咽腔試料との質の相違を反映している可能性があります。
結論
To date, studies assessing the utility of different patient samples for the diagnosis of COVID-19 have largely been conducted on inpatients with known COVID-19 infection (1, 4). Here, we demonstrate feasibility, acceptability and scalability of prospectively collecting saliva from ambulatory patients in a busy screening clinic, and further demonstrate the value of saliva as a non-invasive specimen for the detection of SARS-CoV-2. Although the sensitivity of saliva as a diagnostic specimen is less than NPS, saliva testing may be a suitable alternative first-line screening test in several environments, including low resource settings, with NPS reserved for patients with an ongoing high clinical index of suspicion. These findings are highly relevant in the face of shortages of both swabs and personal protective equipment in many settings (5).
結構な確率で検出できたので唾液は簡便で鼻咽腔の検査よりも安全なので、スクリーニングとしてかなり有用ではないかという感じで書いてます。ただし、鼻咽腔の方がウイルス量が多く検出率が高い事から、臨床的に疑いが強い場合は鼻咽腔も採取する方が良いのではないかという結論になっています。
まとめ
新型コロナウイルスの拡散スピードの速さは、症状発現時からウイルスが鼻咽腔や唾液に発現しており、それが密接な距離での会話等で伝播する事が原因であると以前の論文に書いてありました。
たしかに図をみると、症状発現0日からRT-PCRで検出されています。しかも症状発現から日数が経つとCt値が大きくなっていってます。これはPCRによる増幅回数が増えている、つまり元のウイルス量が減っている事になります。単純にウイルス量だけで拡散力が決まるなら症状発現時にはもうだいぶ拡散力が強い、ということになりそうです。恐ろしいですね。
ということはなんか今日ぐらいからなんか風邪かも?なんていう患者さんを診療してしまうとそれが最も感染力が高い、という事になりそうなので、やはりちょっとでも体調に異変がある方は歯科は診療しない、そこはもう心を鬼にするという方向性がお互いにとってよいのかな?と思いました。