虫歯リスクが高い子供は10代後半~20代前半に注意
日歯生涯研修セミナーを受講
12/16に広島で行われました日本歯科医師会生涯研修セミナーを受講してきました。
広島に行かずとも今年からはネット配信で地元で受講することができます。
文明の利器凄いです。
今回は広島の直接受講の他に記憶が正しければ香川、鳥取、島根、山口、鹿児島、高知がネット受講しました。
午前中は虫歯に関する講義
午前中は大阪大学歯科保存教室の林美加子先生による虫歯の話を受講しました。
虫歯の診断基準やガイドライン、MTAという材料などについてエビデンスを交えながらとてもわかりやすいご講演でした。
紹介された論文の中で気になったものがあったので読んでみることにしました。
Broadbentの報告
Broadbent et al. Trajectory Patterns of Dental Caries Experience in the Permanent Dentition to the Fourth Decade of Life. J Dent Res 87:69-72, 2008.
2008年のニュージーランドの論文です。この論文自体はフリーで入手可能です。
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2254448/
虫歯がどのように発生していくかを1000名近くの被験者において赤ちゃんから経時的に30年以上追った研究であり、かなりレアな研究と言えるでしょう。
Abstract
Dental caries is a chronic, cumulative disease, but no studies have investigated longitudinal patterns of caries experience. The objective of this study was to identify and describe developmental trajectories of caries experience in the permanent dentition to age 32. Longitudinal caries data for 955 participants in a longstanding birth cohort study were analyzed by trajectory analysis. Three caries experience trajectories were identified by the SAS macro PROC TRAJ; these were categorized as “high” (~ 15%), “medium” (~ 43%), and “low” (~ 42%) DMFS (Decayed, Missing, and Filled
Surfaces). All were relatively linear, although the higher trajectories were more “S-shaped”. This effect disappeared following adjustment for the number of unaffected surfaces remaining at each age, suggesting that, among individuals following a similar caries trajectory, caries rate is relatively constant across time.
虫歯は慢性で累積的な疾患です。しかし、虫歯経験の経年的パターンに関する研究はいまだ存在しません。
本実験の目的は32歳までの完全歯列者における虫歯経験の軌跡を調査するものです。955名の経年的な虫歯のデータを出生コホート研究を用い解析しました。
DMFS(治療した部分や放置している歯の面の総数)が高い群(15%)、中間群(43%)、
低い群(42%)の3つの虫歯のパターンが確認出来ました。
全てのパターンは比較的直線性を示しましたが、高い群はよりS波形を示しました。この効果は同じ様な虫歯の軌跡をもつ個人間においては、それぞれの年代で影響をうけていない残りの表面の数を調整することで消失します(ここよく意味がわかりませんでした)。
虫歯の発生率は各年齢層で 比較的 コンスタントでした。
Methods
The Dunedin Multidisciplinary Health and Development Study (DMHDS) is a longitudinal study of a birth cohort of children who were born at the Queen Mary Hospital, Dunedin, New Zealand, between 1st April 1972 and 31st March 1973 (Silva and Stanton, 1997). Perinatal data were obtained, and the sample for the longitudinal study was first followed up at age 3
yrs (N = 1037), and again at ages 5, 7, 9, 11, 13, 15, 18, 21, 26, and, most recently, at 32 yrs. The current study uses data collected from dental examinations at ages 5, 9, 15, 18, 26, and 32 yrs. The Otago Ethics Committee granted ethics approval for each assessment phase. Over
90% of the cohort self-identify as being of European origin. Study participants gave informed consent prior to inclusion.
1972年の4/1から1973年の3/31までにニュージーランドのクイーンメリー病院で産まれた人が被験者です。
最初のフォローアップである3歳時点ではn=1037でそこから5,7,9,11,13,15,18,21,26、最も最近は32歳でのフォローアップが行われました。
本研究は歯の調査を行った5、9、15、18、26、32歳時のデータを使用しました。
Measurement of Dental Caries
At each age, dental examinations for caries and missing teeth were conducted by calibrated examiners. Before each examination, recording sheets were adjusted to account for teeth that had been missing at the previous assessment. Teeth were examined for dental caries and restorations, with 4 surfaces (buccal, lingual, distal, and mesial) being considered for canines and incisors, and a fifth surface (the occlusal) included for premolars and molars. In a small number of cases where a surface could not be visualized by the examiner, the surface was excluded from the examination (and later analyses). We obtained an estimate of accumulated tooth loss due to caries by observing the presence or absence of each tooth, and by ascertaining the reason for its absence at that age by asking the participant at the time of each examination.Repeat examinations were not possible, because of the logistical constraints imposed by the tightly scheduled assessment that study participants underwent. Dental examiners were not aware of study participants’ socio-economic status (SES) or questionnaire responses at the time of the examinations. Further information on these assessments is available in previous publications (Suckling et al., 1985; Thomson et al., 2000; Broadbent et al., 2006).
虫歯に関しては前歯と犬歯は4面、臼歯部は5面に関して検査を行いました。歯面が見えない場合は検査から除外しました。
検査時に歯が存在するかどうかを観察すること、 被験者に喪失理由を聞くことにより、虫歯による歯の喪失があったかどうかを把握することができました。
(後半省略)
RESULTS
Participation rates in the Dunedin Study have remained high, with 972 study individuals (96%) participating at age 32 yrs, and 932 (92%) participating in the dental examination. Dental caries data were available for 955 individuals at 3 or more of the 6 dental assessment ages, and the
following analyses are restricted to those individuals. The 82 excluded individuals included 48 males (9.0%) and 34 females (6.8%).
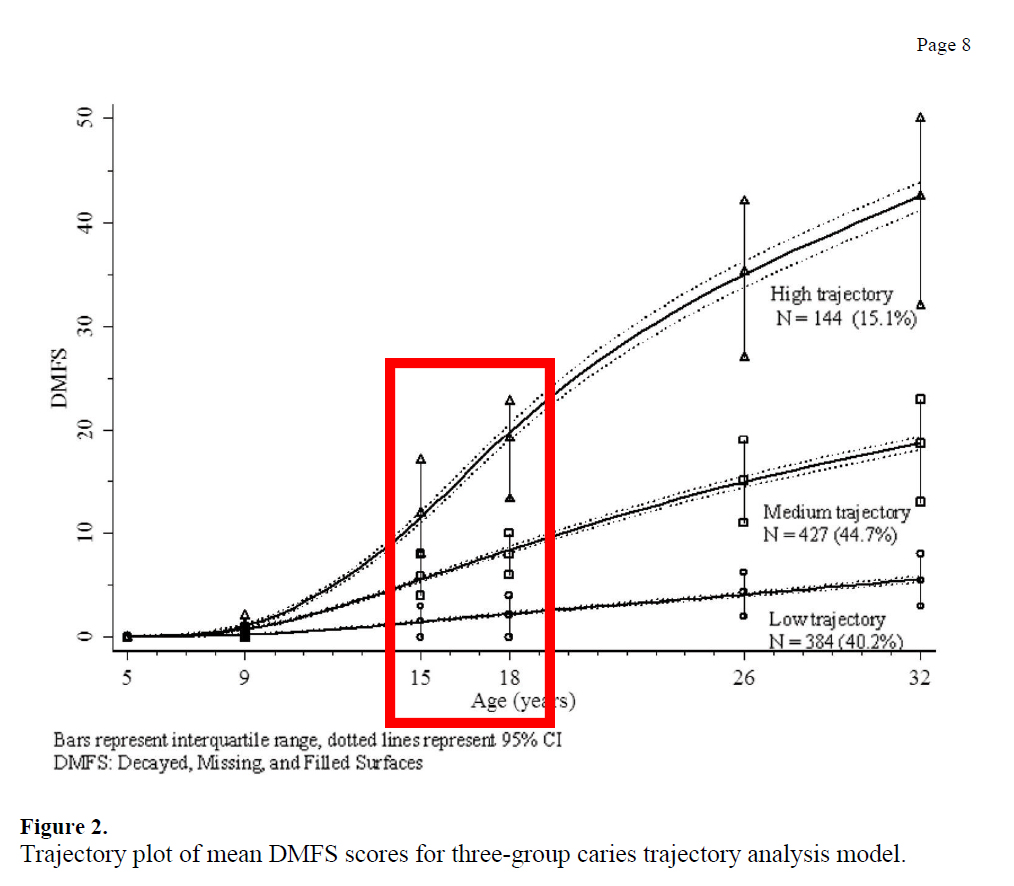
The individual caries trajectories were plotted (Fig. 1), and through the trajectory group assignment based on the PROC TRAJ macro, 384 participants (40.2%) were assigned to ‘group 1’, 427 (44.7%) to ‘group 2’, and 144 (15.1%) to ‘group 3’. These were designated the ‘low’, ‘medium’, and ‘high’ trajectory groups, respectively. When DMFS data by trajectory group were plotted against age, the mean DMFS scores of trajectory groups were seen to diverge with increasing age (Fig. 2). By age 32, the mean DMFS was 5.4 (SD 3.7) in group 1, 18.6 (SD 6.8) in group 2, and 42.3 (SD 12.7) in group 3. On average, 36.9% of tooth surfaces in trajectory
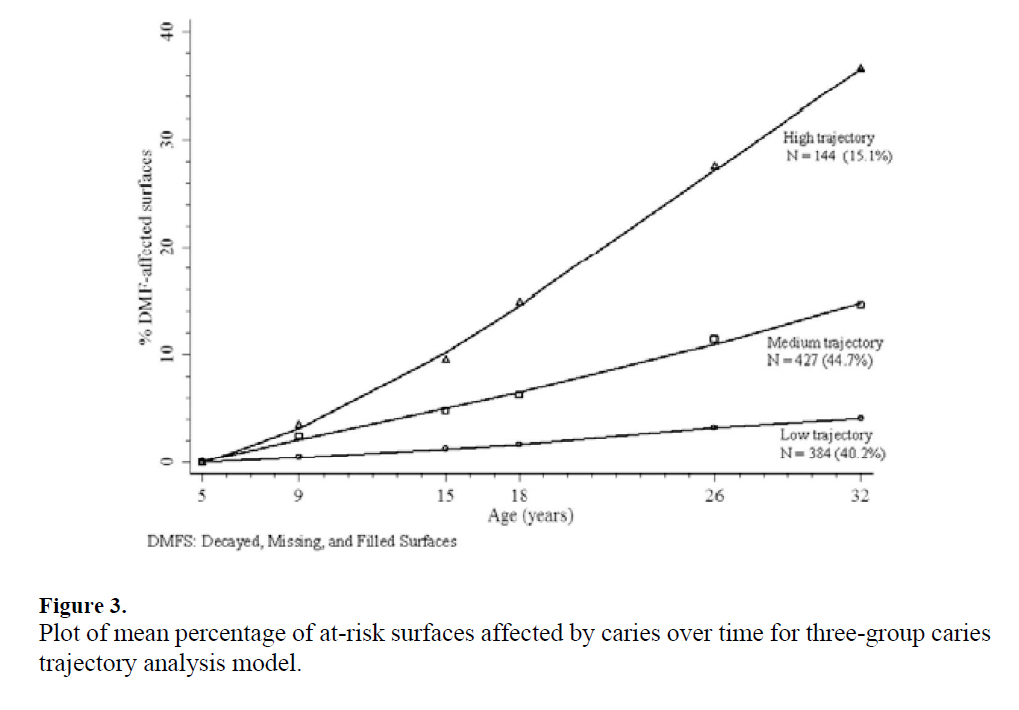
group 3 had been affected by caries by age 32. At the group level, the plot of the percent of caries-affected surfaces (of those permanent teeth present in the mouth) revealed no period of rapid increase in DMF (Fig. 3).
932名の被験者が32歳時の検査に参加しました。虫歯のデータは6回の検査中3回以上参加した955名のデータが使用可能でした。後の82名のデータは欠落となりました。
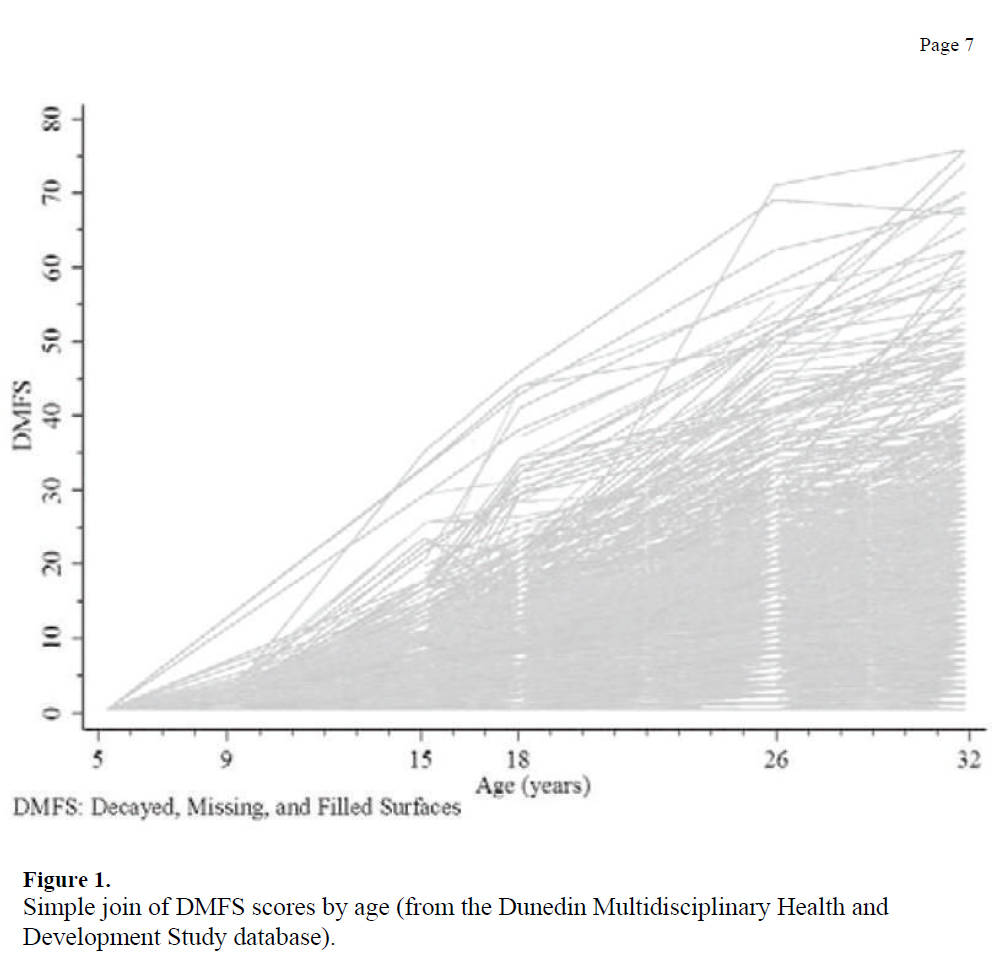
虫歯の遍歴を図1にプロットし、PROCTRAJ macroに基づいて3グループに分類しました。 虫歯罹患が少ない グループ1が384名(40.2%)、中程度のグループ2が427名(44.7%)、多いグループ3が144名(15.1%)に分類されました。グループの各年齢におけるDMFSの平均値は年齢増加によって差が開いてきます。
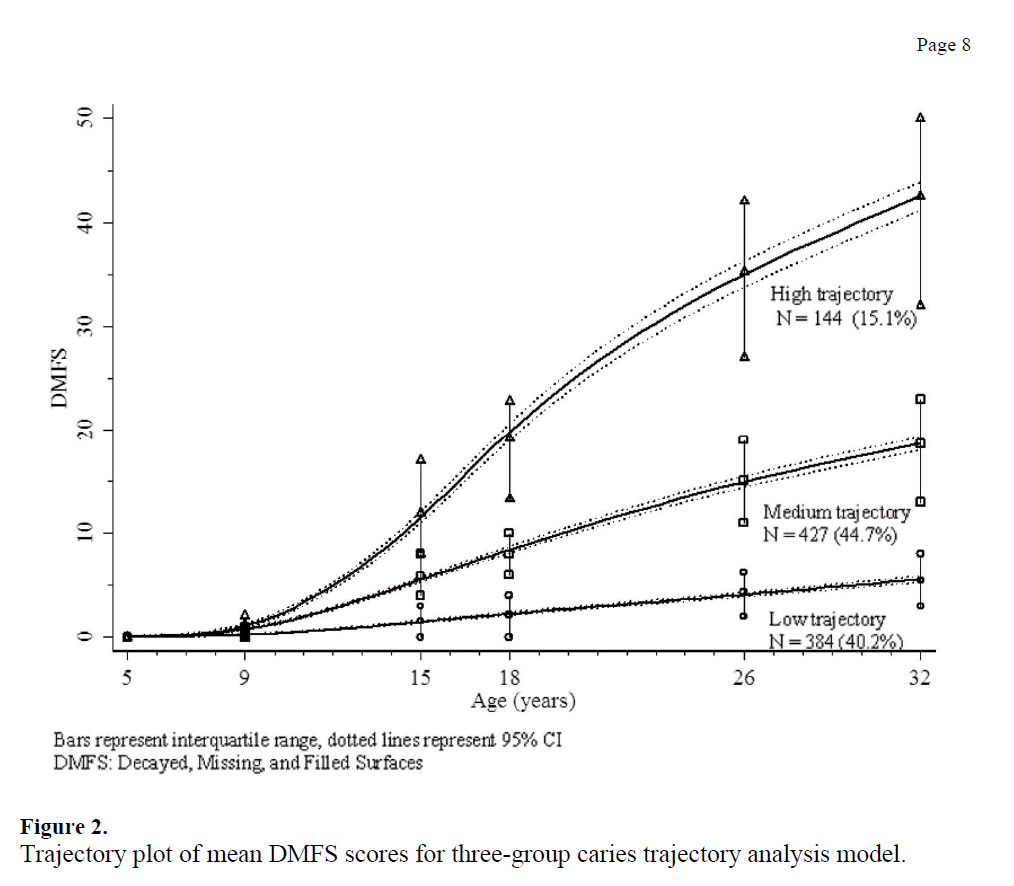
32歳ではグループ1の平均DMFSは5.4(標準偏差3.7)、グループ2の 平均DMFSは18.6(標準偏差6.8)、グループ3の 平均DMFSは42.3(標準偏差12.7) となりました。グループ3では歯面の36.9%に虫歯の影響が認めました。このグループでは加齢による虫歯が影響する歯面の増加に歯止めがかかっていません。
DISCUSSION
The Dunedin Study remains the only dental study to have followed a group of individuals from birth to adulthood. Our use of group-based trajectory analysis appears to be a valid approach to exploring developmental trajectories; the technique has the added advantage of being simple
to interpret. The trajectory groupings are a useful statistical device for capturing the essential features of the underlying complex reality of the longitudinal caries data-set.
A possible weakness of this study is that we have chosen to limit our analyses of possible determinants of trajectory group membership (at this stage), and have not yet considered any potential confounding variables. From an analytical standpoint, it is important to remember that the trajectory ‘groups’ do not exist in the real sense; they are an analytical convenience. Furthermore, several alternative programs are available for estimation of such latent classes (PROC TRAJ, MPlus, and LatentGold), and the outcomes of latent class analyses may differ according to the precise estimation parameters that are specified. PROC TRAJ (which we have
used) does not consider growth factor variances within trajectory classes, while the alternative program MPlus does. This consideration is important theoretically, since it may affect the trajectory group membership of a few cases; however, it is unlikely that including such variation would materially affect the overall outcome (and associated inferences) of the analysis.
Trajectory analysis appears to be a useful and valid descriptive tool in the investigation of caries experience across the life-course, and can aid in the recognition of patterns (or trajectories) of caries experience over time. In this study, the two higher trajectory plots were S-shaped (or cubic), while the lowest trajectory was linear. Teeth were lost at a proportionally greater rate among participants following higher trajectories, thus decreasing the number of surfaces available and ‘at risk’ to caries in the mouth over time. The rate of increase in %- DMFS appeared to be linear in all trajectory groups, with no apparent drop-off in the rate of increase in %-DMFS with increasing age. Thus, analysis of our data does not support the commonly held belief among dentists that childhood and adolescence are periods of special risk for dental caries, or that caries ‘immunity’ may be acquired during late adolescence or early adulthood (Carlos and Gittelsohn, 1965). In this population at least, new caries appears to be occurring at a relatively constant rate, implying that for greatest benefit, caries-preventive measures are necessary at all stages of the life-course.
考察はこの実験手法の限界等について語られており、訳はつけません。
注目点
注目点はやはり虫歯リスクが高い群の伸びではないでしょうか?
他の2つの群と比較すると15歳~18歳で虫歯の増加角度が急になりそれ以降はやや変曲点を描いて落ち着きますが、それでも32歳時では他の2群と相当な差を認めます。
それに比べて中間グループと虫歯リスクが低いグループはほぼ直線的に虫歯の歯面が増えているようにみえます。
基本的にこの実験では家庭環境等までは考慮されていないので、なんともいえませんが要因はいくつか考えられます。
幼い頃は親が仕上げ磨き等をしますが、15歳でまだ仕上げ磨きしてもらっている人はほぼいないでしょう。
また15歳ともなれば友達づきあいが多くなり、食生活や生活リズムも変わってくると考えられます。高校を卒業すれば1人暮らしすることもあるでしょう。
そういった事が原因で虫歯にただでさえなりやすい群は一気に虫歯が増えてしまうのではないでしょうか?
日本の場合は?
日本の場合、虫歯で大規模な調査というと6年に1回行われている歯科疾患実態調査がまず思い浮かびます。
ただ、この調査ですが、各年齢階層で人数にばらつきが多く、どこまで信頼できるかは微妙なところです。

虫歯をもつ者の割合をみてみると、10~14歳では虫歯にかかったことがある人はかなり少ないですが、15~19歳ではグンと増えています。さらに20代になるともう虫歯になったことがない人の方がマイノリティになります。
歯科疾患実態調査からみても10代後半で虫歯にかかる子供が多いのは確かなようです。
まとめ
この文献から考えると
①10歳前半までの虫歯を極力少なくする。
もともとリスクが高くなければよいわけですから、乳歯の虫歯はないようにとかそういった事を考える必要があります。ということは子供の頃は特にお母さんを啓蒙する必要がありそうです。
②虫歯のリスクが高めの子供は10代後半においてもメンテナンスプログラムを組む。メンテナンスプログラムは20代においても継続することが望ましい
リスク高めの子は15歳ぐらいからさらに加速するわけですから、歯磨き指導やフッ素塗布など定期的な管理は絶対必要でしょう。
ただし、虫歯のリスクが高い子はなぜ高いか、と言われれば歯に興味がなかったり、歯医者さんになかなか来なかったりなんですよね・・・。難しいです。
この論文をうまく啓蒙に取り入れて実際の臨床に反映できればよいなあ、と思います。